Dobutamine Stress Echocardiography
The Complete Clinical Guide for Cardiologists, Surgeons & Physicians
What is Dobutamine Stress Echocardiography?
Dobutamine Stress Echocardiography (DSE) is a pharmacological cardiac stress test that uses intravenous dobutamine — a synthetic catecholamine — to incrementally increase heart rate and myocardial contractility, thereby simulating the physiological demands of physical exercise.
Simultaneous echocardiographic imaging captures real-time wall motion at each stage, enabling detection of inducible ischaemia, assessment of myocardial viability, and evaluation of valvular haemodynamics under stress.
DSE is the preferred modality for patients who cannot perform adequate exercise on a treadmill or bicycle — including those with orthopaedic limitations, peripheral vascular disease, severe deconditioning, or neurological impairment.
How DSE Works
Why is DSE Performed?
Dobutamine stress echocardiography addresses four major clinical questions in non-invasive cardiology.
CAD Detection
Detects flow-limiting coronary artery disease by provoking inducible wall motion abnormalities under graded dobutamine infusion, identifying territories supplied by stenotic coronary arteries.
Myocardial Viability
Differentiates viable (hibernating or stunned) myocardium from irreversibly scarred tissue using the biphasic response — contractile reserve at low-dose dobutamine predicts functional recovery after revascularisation.
Pre-Operative Risk
Stratifies perioperative cardiac risk before major non-cardiac surgery in patients with limited functional capacity, guiding anaesthetic planning and the decision to proceed, optimise, or revascularise.
Valve Disease Assessment
Evaluates haemodynamic significance of valvular stenosis (particularly low-flow, low-gradient aortic stenosis) and unmasks latent severity by augmenting transvalvular flow under pharmacological stress.
The Dobutamine Stress Echo Protocol
A graded pharmacological stress test that incrementally increases myocardial oxygen demand to unmask flow-limiting coronary disease.
Record resting images in all standard views (PLAX, PSAX, A4C, A2C). Document baseline heart rate, blood pressure, and 12-lead ECG. Assess resting wall motion in all 17 segments.
Begin dobutamine infusion. At this dose, look for augmentation of hypokinetic or akinetic segments — a hallmark of myocardial viability. Monitor for early chronotropic response.
Continue monitoring for viability response (biphasic response). Segments that improve at low dose but worsen at peak dose suggest hibernating but viable myocardium with significant stenosis.
Heart rate begins to rise significantly. New or worsening wall motion abnormalities at this stage suggest inducible ischemia. Acquire images at each stage for comparison with baseline.
Increased inotropy and chronotropy. Closely monitor for new regional wall motion abnormalities, significant arrhythmias, or symptoms (chest pain, severe dyspnea). BP may begin to drop.
Maximum infusion rate. If target heart rate (85% of age-predicted max) is not achieved, Atropine may be added (see note). Acquire peak stress images immediately. This is the most sensitive stage for ischemia detection.
Stop dobutamine infusion. Record recovery images as heart rate declines. Monitor until heart rate and blood pressure return toward baseline. Watch for delayed ischemia or arrhythmias during this phase.
Who Needs a Dobutamine Stress Echo?
Primary Candidates
- Patients unable to achieve adequate exercise capacity (≥85% age-predicted max HR) on a treadmill or bicycle
- Suspected coronary artery disease in patients with orthopaedic, neurological, or peripheral vascular limitations
- Assessment of myocardial viability in chronic ischaemic left ventricular dysfunction before considering revascularisation
- Pre-operative cardiac risk stratification prior to major non-cardiac surgery in patients with poor functional capacity
- Evaluation of haemodynamic significance of valvular heart disease, especially low-flow low-gradient aortic stenosis
- Follow-up assessment of known coronary artery disease when exercise testing is inconclusive or not feasible
Important Considerations
- Patients with left bundle branch block (LBBB) may show false-positive septal wall motion abnormalities — vasodilator stress (adenosine or regadenoson) is generally preferred in this population
- Dobutamine is contraindicated in patients with severe uncontrolled hypertension, recent acute coronary syndrome, or significant ventricular arrhythmias
- Concomitant beta-blocker therapy should be withheld (typically 24–48 hours) prior to the study to allow adequate chronotropic response
- Patients with pacemaker-dependent rhythms may require alternative stress modalities depending on the clinical question
Contraindications & Safety Considerations
Prior to performing DSE, clinicians must carefully screen patients for absolute and relative contraindications to ensure patient safety.
Absolute Contraindications
- Acute myocardial infarction (within 2 days)
- Unstable angina not yet stabilised with medical therapy
- Left ventricular outflow tract (LVOT) obstruction
- Hypertrophic obstructive cardiomyopathy (HOCM)
- Severe uncontrolled hypertension (systolic >180 mmHg or diastolic >100 mmHg)
- Known hypersensitivity or allergy to dobutamine
- Significant ventricular arrhythmias (sustained VT, VF, or multifocal PVCs at rest)
Relative Contraindications
- High-degree atrioventricular (AV) block without a functioning pacemaker
- Sick sinus syndrome without a functioning pacemaker
- Resting systolic blood pressure <90 mmHg
- Significant electrolyte imbalance (especially hypokalaemia or hypomagnesaemia)
- Known unprotected left main coronary artery (LMCA) stenosis
- History of ventricular tachycardia (non-sustained or controlled)
Interpreting Stress Echo Results
Understanding the five major result categories of dobutamine stress echocardiography and their clinical implications.
New or worsening wall motion abnormalities (WMA) during stress, indicating flow-limiting coronary artery disease. Typically warrants coronary angiography for further evaluation.
Normal augmentation of wall motion at peak stress with no new regional abnormalities. Excellent negative predictive value — annual cardiac event rate < 1% for the following 1–3 years.
Borderline or technically inadequate result, often due to sub-optimal image quality, failure to reach target heart rate, or isolated basal inferior hypokinesis. May require alternative imaging (e.g., nuclear perfusion or CMR).
Low-dose dobutamine augments contractility in akinetic/hypokinetic segments, suggesting hibernating but viable myocardium. Biphasic response (improvement at low dose, worsening at high dose) is the strongest predictor of recovery post-revascularization.
No augmentation at any dobutamine dose in akinetic segments, indicating transmural scar. These segments are unlikely to benefit from revascularization; medical therapy is preferred.
AHA 17-Segment Bullseye Model — Interactive wall-motion scoring mapped to coronary artery territories. Each segment is graded 1 (normal) through 5 (dyskinetic).
Why You Should Order a DSE Before Surgery
Reduce Perioperative Events
Identify patients at high risk for perioperative MI, heart failure, or death before they reach the operating room. DSE detects inducible ischemia and assesses ventricular function under hemodynamic stress — information that directly changes surgical planning and anesthesia strategy.
ACC/AHA Guideline Recommended
The 2014 ACC/AHA Perioperative Guideline recommends pharmacological stress testing for patients with elevated risk (RCRI ≥ 3) and poor functional capacity (< 4 METs) undergoing vascular or high-risk non-cardiac surgery. DSE is a Class IIa recommendation in this setting.
Beyond ECG Alone
Resting ECG and clinical assessment miss up to 50% of patients with significant CAD. Dobutamine stress echo provides real-time visualization of wall motion under stress — offering superior sensitivity and specificity compared to exercise ECG for patients who cannot exercise.
Standardize Your DSE Workflow
Everything you need for a safe, efficient, and well-documented dobutamine stress echo — in one free, privacy-first web app.
Dobutamine Calculator
Auto-calculate infusion rates based on patient weight and target dose. Supports concentrations from 250 mg/250 mL to custom preparations with real-time mL/hr output.
Per-Stage Monitoring
Track heart rate, blood pressure (systolic/diastolic), symptoms, ECG changes, and wall motion at every dobutamine stage with auto-populated protocol timings.
AHA 17-Segment Model
Interactive bullseye display for grading wall motion across all 17 myocardial segments, mapped to LAD, LCx, and RCA coronary territories.
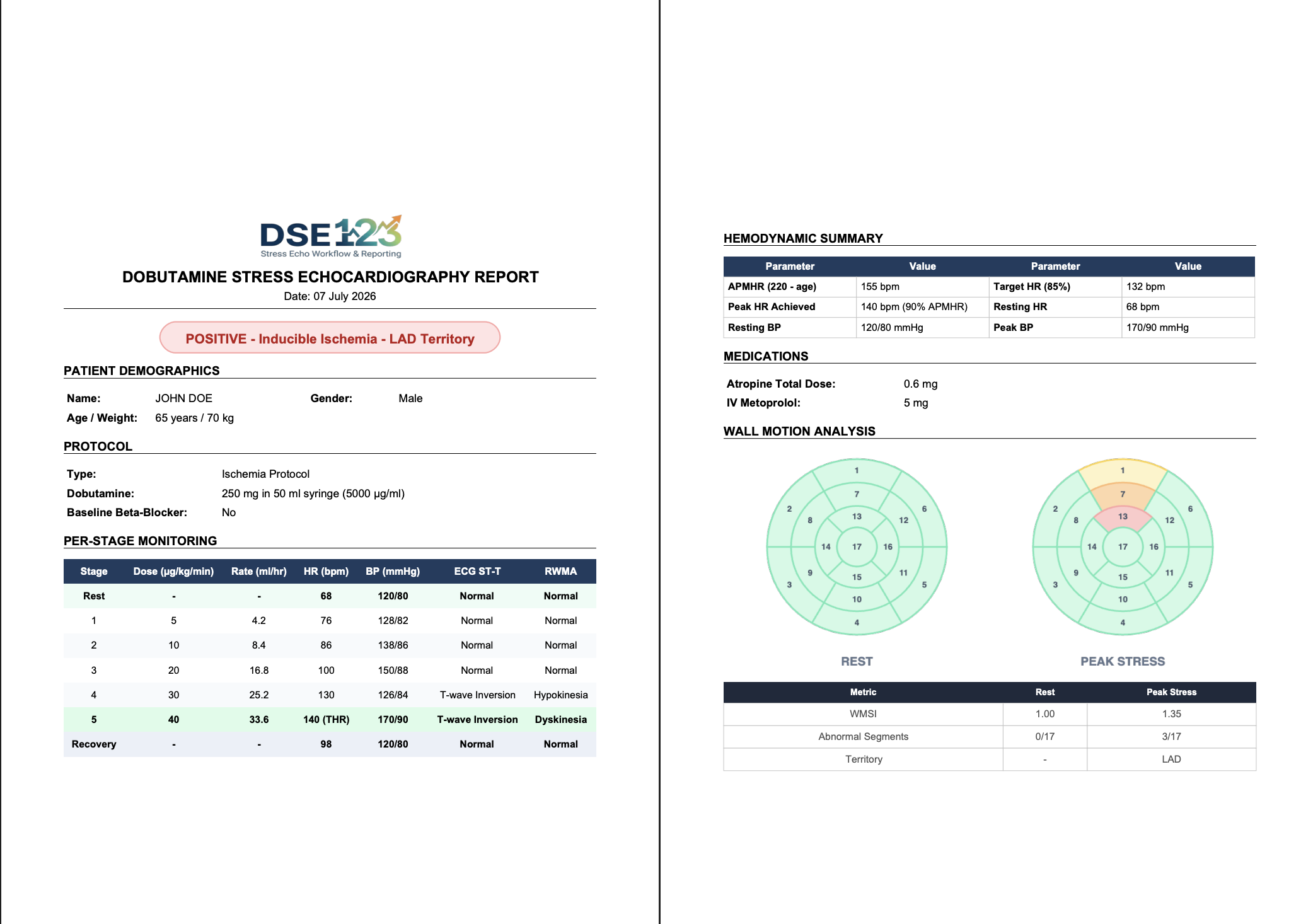
PDF Reports
Generate structured, print-ready PDF reports with full hemodynamic data, wall motion grading, and clinical conclusions — ready for EMR upload or fax.
Three Protocols
Standard, accelerated, and viability-focused dobutamine protocols with automatic stage progression and customizable dose increments per ACC/AHA guidelines.
Privacy by Design
All patient data stays on your device. No cloud uploads, no accounts required, no tracking. HIPAA-conscious architecture with zero data persistence beyond your session.
Sample Report Preview
Everything You Need to Know About DSE
Dobutamine Stress Echocardiography is a pharmacological stress test that uses intravenous dobutamine — a synthetic catecholamine — to incrementally increase heart rate and myocardial contractility while echocardiographic images are recorded. It evaluates left ventricular wall motion at rest and at peak stress to detect inducible ischemia, assess myocardial viability, and quantify the hemodynamic severity of valvular heart disease, particularly in patients who cannot exercise adequately.
A typical DSE procedure takes approximately 30–45 minutes from start to finish. The dobutamine infusion itself follows a staged protocol — usually starting at 5 µg/kg/min and increasing every 3 minutes up to 40 µg/kg/min, with atropine added if needed to reach 85% of age-predicted maximum heart rate. Preparation (IV access, baseline imaging) adds about 10–15 minutes, and post-stress monitoring continues until heart rate and blood pressure return to near-baseline values.
DSE has an excellent safety profile with serious adverse events (sustained ventricular tachycardia, myocardial infarction, or death) occurring in fewer than 1 in 2,000 tests. Common transient effects include palpitations, mild chest discomfort, and flushing, all of which resolve quickly once the infusion is stopped. The test is performed under continuous ECG monitoring with resuscitation equipment and reversal agents (esmolol) immediately available, and is supervised by a physician trained in advanced cardiac life support.
Exercise stress echocardiography is generally preferred because it provides additional prognostic data (exercise capacity, heart rate recovery, blood pressure response). However, many patients — including those with severe arthritis, peripheral vascular disease, neurological impairment, morbid obesity, or deconditioning — cannot achieve adequate exercise workload. Dobutamine provides a reliable pharmacological alternative that mimics exercise-induced hemodynamic stress, allowing accurate assessment of wall motion and valve gradients without requiring physical exertion.
The most common side effects are palpitations (feeling your heart beat fast or hard), mild chest tightness, flushing, headache, and a warm sensation. Some patients experience brief nausea or dizziness at higher doses. These effects are expected, transient, and directly related to dobutamine's stimulatory action on the heart. They resolve within minutes of stopping the infusion. Serious arrhythmias or hypotension are rare and are managed immediately by the supervising physician with appropriate medications.
Your doctor will instruct you to stop beta-blockers (e.g., metoprolol, atenolol) at least 24–48 hours before the test, as they blunt the heart rate response and can render the test non-diagnostic. Avoid caffeine, theophylline, and other stimulants for 24 hours. You may eat a light meal but should avoid heavy meals 2–3 hours prior. Bring a list of your current medications, and wear comfortable, loose-fitting clothing with easy access to your chest for electrode and ultrasound probe placement.
A positive DSE result indicates that new wall motion abnormalities appeared during stress — meaning one or more segments of the heart muscle did not contract normally at higher heart rates. This suggests significant coronary artery disease causing inducible ischemia in the territory of the affected artery. Your cardiologist will correlate these findings with your symptoms, risk factors, and other investigations to determine whether further evaluation (such as coronary angiography) or medical optimization is warranted.
Current ACC/AHA and ESC guidelines recommend preoperative DSE for patients undergoing elevated-risk non-cardiac surgery (e.g., major vascular, intra-abdominal, or intrathoracic procedures) who have poor functional capacity (less than 4 METs) and one or more clinical risk factors — such as history of ischemic heart disease, compensated heart failure, cerebrovascular disease, diabetes mellitus, or renal insufficiency. The test helps stratify perioperative cardiac risk and guide the decision between proceeding with surgery, medical optimization, or coronary revascularization.
At low-dose dobutamine (5–10 µg/kg/min), viable but dysfunctional myocardium ('hibernating' or 'stunned' myocardium) shows improved contractility — a response known as contractile reserve. If these same segments then deteriorate at higher doses (biphasic response), this pattern has high predictive value for functional recovery after revascularization. DSE is one of the most validated and widely available methods for viability assessment, alongside cardiac MRI with late gadolinium enhancement and nuclear perfusion imaging.
DSE123 is a purpose-built clinical decision-support tool designed to streamline the entire Dobutamine Stress Echo workflow. It guides clinicians through a structured 3-step process — Step 1 (Pre-test): patient selection, contraindication screening, and risk stratification; Step 2 (During Test): real-time protocol tracking with dose/stage calculations and endpoint monitoring; Step 3 (Post-test): standardized reporting with wall motion scoring and guideline-concordant interpretation. Built by a practicing interventional cardiologist, it reduces protocol errors, ensures guideline adherence, and produces professional reports in minutes.
Understanding Your Stress Echo Test
What to Expect
How to Prepare
- ✓Stop beta-blockers 24–48 hours before (as directed by your doctor)
- ✓Avoid caffeine and energy drinks for 24 hours
- ✓No heavy meals 2–3 hours prior to the test
- ✓Wear loose, comfortable clothing
- ✓Bring a list of all your current medications
- ✓Arrange for someone to drive you home if you feel unwell
Common Side Effects
When to Contact Your Doctor
- ⚠Prolonged chest pain lasting more than 15 minutes after the test
- ⚠Severe shortness of breath or difficulty breathing at rest
- ⚠Fainting or near-fainting episodes
- ⚠Irregular or very rapid heartbeat that does not settle
- ⚠Swelling in your legs, ankles, or feet
Guideline References & Citations
Pellikka PA, Arruda-Olson A, Chaudhry FA, et al. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J Am Soc Echocardiogr. 2020;33(1):1–41.e8.
Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur Heart J. 2022;43(7):561–632. (Updated 2025 Focused Update).
Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143(5):e72–e227.
Baumgartner H, Hung J, Bermejo J, et al. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30(4):372–392.
Lancellotti P, Pellikka PA, Budts W, et al. The Clinical Use of Stress Echocardiography in Non-Ischaemic Heart Disease: Recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30(2):101–138.
Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e199–e267.
Clavel MA, Magne J, Pibarot P. Low-Gradient Aortic Stenosis. Eur Heart J. 2016;37(34):2645–2657. Clavel MA, Burwash IG, Pibarot P. Cardiac Imaging for Assessing Low-Gradient Severe Aortic Stenosis. JACC Cardiovasc Imaging. 2017;10(2):185–202.

Dr. Kunal Ajay Patankar
MBBS, MD, DrNB (Cardiology)
Interventional Cardiologist · HVS Hospitals, Mumbai
Dr. Patankar built DSE123 to bridge the gap between complex guideline recommendations and everyday clinical workflow. Drawing from hands-on experience performing and interpreting dobutamine stress echocardiograms in a high-volume cardiac center, he designed DSE123 as a structured decision-support tool that reduces protocol variability, minimizes documentation burden, and helps clinicians deliver standardized, guideline-concordant care — from patient selection through final reporting.
Medical Disclaimer: DSE123 is an educational and clinical decision-support tool. It does not replace independent clinical judgment. All patient management decisions must be made by qualified healthcare professionals based on individual clinical assessment. The content on this page is for informational purposes only and is based on published guidelines and peer-reviewed literature.